


Elise M. Weerts, Ph.D., a behavioral pharmacologist, neuroscientist, and professor of psychiatry and behavioral sciences at Johns Hopkins Medicine, is one of the women who have spent their careers closing that gap. Jacquie first spoke with Dr. Weerts in October 2018, just as the platform launched and as she was beginning a clinical PET-imaging study of cannabis withdrawal in women, work designed specifically to address the absence of female subjects in the earlier imaging literature. More than seven years later, Jacquie sat down with Dr. Weerts again to revisit that study, “Sex differences in cannabis withdrawal symptoms among treatment-seeking cannabis users”, and examine how the research and regulatory landscape and the place of women within it have and have not changed.
“Most women find it challenging at the beginning. It’s better than it was 25 or 50 years ago, but it’s still a work in progress.”
— Elise M. Weerts, PhD
Women are still a minority in cannabis science, both as the researchers doing the work and as the subjects it studies. Much of the foundational human research on cannabis was conducted almost entirely in men, and the ranks of scientists investigating it have long skewed the same way. There aren’t very many of us.
JCR: When did you start researching cannabis?
EW: I had to think back on that one. Somewhere in the mid-2010s. I actually started my career studying alcohol; I began seeing a lot of cannabis use in people who were drinking alcohol. As I watched cannabis emerge as the next major substance moving toward broad public use, much the way alcohol had, I shifted into studying cannabis too. That’s how it happened.
JCR: For your studies, where are you sourcing cannabis? Are you still using the Ole Miss material?
EW: We’ve continued to source from the NIDA Drug Supply Program, which is the Ole Miss source, and it still has supply. That has worked well for us for a simple reason: it all runs through the Drug Enforcement Agency (DEA) and the National Institute on Drug Abuse (NIDA). The products are tested, we have certificates of analysis (COA), and antimicrobial testing is done so we know there’s no mold or other contaminants. State laws have changed, but federal law hasn’t changed in the same way, and the two don’t align; we’re obligated to follow federal law. We still answer to the federal framework. More recently, FDA-approved marijuana products and products containing marijuana subject to a qualifying state-issued license was moved from Schedule I to Schedule III per the president’s executive order, but I haven’t seen that functionally change what I do.
I’d also push back on some of comments about NIDA cannabis products being a mediocre product. In reality, NIDA drug supply offers multiple varieties, multiple versions, and different concentrations: THC-dominant cannabis, CBD-dominant cannabis, balanced forms with equal THC and CBD, and, importantly, a cannabis placebo so we can run placebo-controlled trials. The program also provides full-spectrum extracts and purified minor cannabinoids such as Delta-8, CBG, and CBC. That lets us systematically test products we know are as labeled, and without contaminants.
JCR: With state laws shifting and the move toward Schedule III, how does access look for researchers, medical cannabis patients, and cannabis consumers?
EW: The regulatory landscape is constantly changing, which is challenging for research because we can’t simply access what the average consumer can. I also feel for medical cannabis patients and consumers, because what they receive isn’t consistent from visit to visit. In Maryland, for example, the dispensaries, which aren’t pharmacies, though the labeling rules treat them somewhat like one, are required to itemize weight, cannabinoids, and terpenes. In practice, the labels generally list only THC, CBD, THCA, CBDA, and a few major terpenes. The full profile is supposed to be available, but it’s typically accessible only through a QR code, a web link, or a peel-back label, so the consumer has to go do the research themselves. It could be more transparent.
JCR: Who can actually supply cannabis for research?
EW: To supply cannabis for research, a company must be a DEA-approved bulk manufacturer and supplier. I’m aware of seven companies that were approved but of those, I’m not aware of any actually providing cannabis plant material to researchers. There has been discussion of one biopharmaceutical research company supplying finished products—edibles and oils—rather than plant material. When I tried to look some of the others up, I couldn’t even find a website, which made me wonder whether they’re still operating.
The registration process is demanding. A company has to register with the DEA, hold a bona fide supply agreement, secure a production quota, provide advance notification and invoicing, and then give notification at harvest and transfer of ownership, all of which loops back to the DEA.
JCR: There’s a consumer belief that higher THC means a better product. What has happened to THC concentrations?
EW: Concentrations of THC have climbed steadily. Think back to the early 1980s; flower was around 3 or 4% THC. Now, a great deal of flower is 30% or 34%, and with vapes, concentrates and similar products, you can reach essentially pure THC, around 95%.
JCR: Is there a biological ceiling, a point where more THC stops producing a stronger effect?
EW: I don’t know, and I don’t believe those studies have been done. The only way to know would be a PET imaging study in which you saturate the receptor, and I can’t see how you’d accomplish that.
What is a PET scan? Positron emission tomography (PET) is an imaging method that measures biological activity rather than anatomy. Researchers introduce a tiny tracer amount of a radioactive compound designed to bind one specific target, in this case the CB1 cannabinoid receptor, and the scanner maps where, and how much of, that target is present in the living brain. It is what lets Dr. Weerts compare receptor density between men and women, and before and after a period of abstinence.
JCR: From hypothesis to publication, how long does a study like your PET work take?
EW: The PET study was about a two-year project. It was funded as an R21, a small developmental grant from NIH, not a large R01, so it was limited in scope, which is why it’s a short comparison. We had just started it when you and I first spoke in October 2018; it wasn’t yet complete. The paper was published in 2021 after completing the study.
JCR: What made your study different from the earlier PET imaging work?
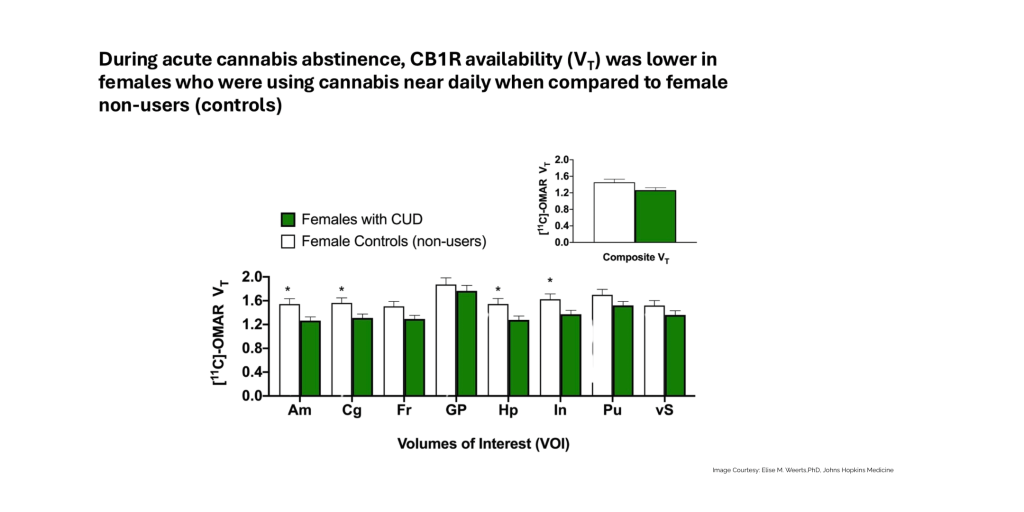
EW: The earlier PET studies of the cannabis type-1 receptor in people who use cannabis were essentially all males; the studies by Hirvonen (2012) and D’Souza (2016), for instance, had no females, and I believe one other study (Ceccarini 2013) included only two women. We made a point of including women, and we built in two key controls. First, we fixed the time from last cannabis exposure: participants came in, completed a standardized smoking session, and then entered the clinical research unit for three days of abstinence, so everyone was in exactly the same state at the time of imaging. The earlier studies imaged at 24-hour post-admission, but you didn’t actually know when those participants had last smoked, which could have introduced a lot of variability.
Second, we controlled for the women’s estrous cycle: PET scans were within the first 14 days after their period and biologically confirmed that they were in the follicular phase . Third, historical controls were selected to match age and BMI ranges for women with cannabis use disorder.
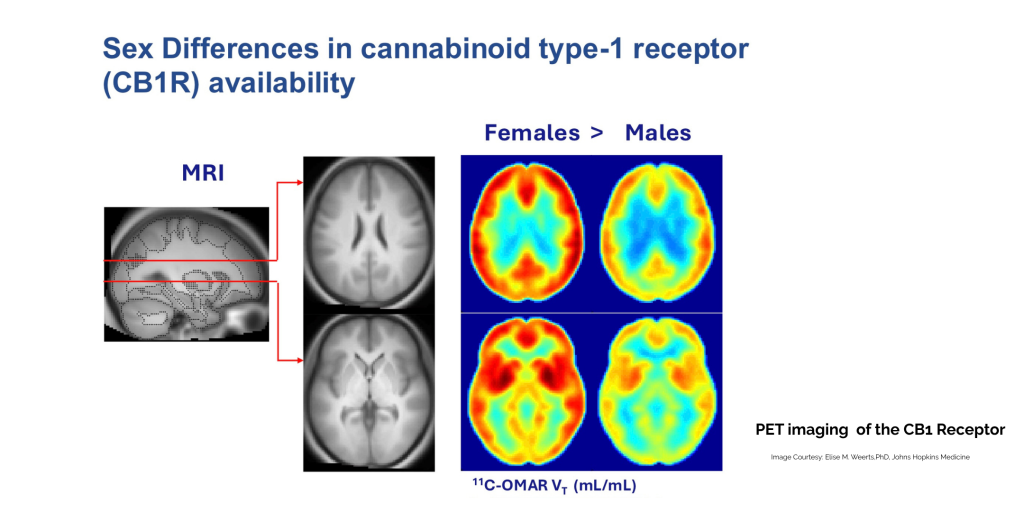
JCR: The difference in CB1 receptor density between men and women is fascinating. Is it true that women’s CB1 receptors increase with age while men’s decline?
EW: I’d have to check that, because I don’t do the aging research. But across my preclinical animal work and my human clinical studies, females tend to be more sensitive to some of the effects of THC. Together with my colleagues in the our cannabis science lab led by Dr. Ryan Vandrey, we have examined sex effects across different routes of administration, such as vaporized versus oral THC, and you can see differences in how men and women respond: in how much effect they feel, in the pharmacokinetics, meaning how much drug is detected in the blood, and in the pharmacodynamics, meaning the behavioral outcomes such as sedation, stimulation, and cognitive processing. My colleagues Tori Spindle leads our driving studies, which show how cannabis affects driving ability when consumed alone or in combination with alcohol.
Women also show a faster trajectory from first use to problematic use; they reach the point of seeking treatment sooner than men. Men still represent the larger share of people in treatment, but the women progressed to needing treatment more quickly, and that may be related to sex differences in receptor density and downregulation of the receptor with chronic use. Women are often more difficult to treat for cannabis use disorder.
I want to be careful, though; it isn’t right to say there are only differences. There are many similarities. Often the difference is in the time course of effects, in when the peak hits and how the drug is metabolized, rather than in the ultimate outcome. It’s true for other drugs, too. Women generally have smaller body size, more body fat, and higher body water, so with alcohol, for example, we reach the same blood concentration with fewer drinks. Similarly, women can show higher blood THC at the same dose as men, and you have to account for that.
JCR: Many non-flower products are sold at standard doses rather than by body weight. Does a woman taking a gummy experience it differently from a man?
EW: These products generally aren’t dosed milligram-per-kilogram or by body water; they’re sold at a standard concentration. In research, we can adjust for body weight, and that’s exactly where controlled dosing teaches you a great deal.
JCR: THC is stored in fat, and women carry more body fat. Is there a correlation in how long THC stays in the body?
EW: Someone else likely has that research. I don’t know whether women retain THC longer, or whether THC is stored in fat, re-released more in women. It’s a really interesting question.
JCR: When you research, you’re working with a standardized product, unlike what consumers receive. What does “research-grade” really mean, and how variable is consumer cannabis?
EW: In any study, the product has to be the same product throughout—standardized, with a COA, free of contaminants and mold, and with enough on hand to run the entire study. You also need a matched, inactive placebo that contains the same constituents minus whatever active component you’re studying, and that placebo can include terpenes and flavonoids.
But people forget that cannabis is a plant. Whether it’s grown in the ground or hydroponically, how it’s bred, grown, and stored all affects its chemical composition. For a while, breeders focused on one or another cannabinoid; for example, there was a stretch when some breeders bred for higher CBG, and then the fad shifted. Long-term storage and storage conditions can result in higher concentrations of products such as CBN (Cannabinol) formed during the degradation of THC. So, the product you buy in Colorado is not the product you buy in Massachusetts unless it’s from the same breeder/supplier, at the same time, under the same conditions. And non-flower products, such as edibles, oils, and vape cartridges are often extracts that isolate specific cannabis components or synthetics like Delta-8, Delta-10, and HHC, which vary from product to product.
In studies done here at Hopkins, tested products frequently didn’t contain the amounts listed on the label; sometimes they contained none of the labeled product and sometimes other products that weren’t listed at all. It’s very hard for a consumer to know or trust what’s on the label for many of these products.
JCR: Where are you sourcing the minor cannabinoids, such as Delta-8, Delta-10, and HHC?
EW: From NIDA and also from ElSohly Laboratories. Dr. Mahmoud ElSohly ran the Ole Miss program and still provides these purified products for research from his lab, though at a cost, whereas the NIDA product was provided to researchers for free. We’re still working out how to obtain products for testing: acquiring them, running the COA, and doing the microbial and stability testing. It’s neither easy nor inexpensive.
JCR: As a researcher, what is your greatest hope for an outcome of Schedule III?
EW: I’ll be honest; whether it’s Schedule I or Schedule III doesn’t change much for me. I hold a Schedule I license and a Schedule II-through-V license, so I store the drug the same way, track it the same way, and handle it the same way: chain of custody and DEA 222 forms; it’s simply a matter of which form is used. It is genuinely helpful for people who don’t already have a Schedule I license, and a Schedule III license is easier to obtain, with different storage and inventory requirements. But otherwise, it’s quite similar. The industry’s messaging that “Schedule III means a wholesale easing of restrictions” overstates it; the restrictions are still there.
JCR: What actually makes a drug a “scheduled” drug?
EW: The schedules describe abuse potential and recognized medical use:
- Schedule I, no accepted medical use, and a high potential for abuse. THC was here; heroin still is.
- Schedule II, high abuse potential, capable of severe psychological or physical dependence, but with a recognized medical use. Morphine and Adderall are examples.
- Schedule III, moderate abuse potential. Hydrocodone with acetaminophen is an example.
- Schedule IV, less abuse potential than II or III but more than V, for instance, diazepam.
- Schedule V, low abuse potential, such as codeine cough preparations, in part because they’re oral rather than a pill that could be ground up and injected.
EW: The important nuance is that the DEA regulates the formulation, not the drug itself. Schedule III doesn’t automatically place all THC products there. Once someone submits a specific formulation for a medical purpose, it can carry a lower schedule. Schedule III essentially reflects that a medical use of a specific product formulation is being recognized.
JCR: Is there a particular area of women’s health you’re looking forward to researching, and where is the greatest need?
EW: In both my animal and human work, I always include both sexes, because women are half the population, and you need to know how a drug works in both. It isn’t only about identifying differences. It’s about establishing whether a drug is effective in both sexes, whether it’s more harmful to one sex, and whether it works for the proposed indication in only one sex. It’s reassuring when the findings are similar, because then we don’t have to worry about sex-specific harms.
The logic is the same as being broadly inclusive of different racial and ethnic backgrounds; genetic makeup can influence how people metabolize and respond to drugs. If you study only European Caucasians, you won’t understand how a drug affects the general population, and if you include only men, you won’t understand how it affects women.
JCR: What is the dosage in your PET study?
EW: In PET, the amount of drug in the CB1 radiotracer is a trace amount; it isn’t pharmacologically active. And we don’t use THC; we use a compound that binds to the same receptor THC does. It’s a derivative of Rimonabant, an inverse agonist, once called an antagonist, that was originally developed for eating disorders and later withdrawn. The tracer labels the receptor without producing an effect like THC; participants don’t feel it. The best radiotracer for tagging a receptor is precisely one that produces little to no effects, just enough to bind the receptor, and nothing more.
JCR: So, participants feel the effects of withdrawal but not intoxication?
EW: The radiotracer does not change withdrawal. They feel withdrawal if they’re in cannabis withdrawal, yes, but by day four, symptoms are lower. Withdrawal tends to peak on days two and three; in the male studies specifically on withdrawal, you can see it can extend to day four. We imaged after an abstinence period because we didn’t want any residual cannabis tainting the receptor imaging, but I was interested in the relationship to withdrawal, so I wanted participants near the peak, around day three or four. The women in our study were in withdrawal, but not severely so. They were near daily heavy users, as you can see in the paper, but the withdrawal in this sample wasn’t particularly severe.
JCR: My professional focus includes creating opportunities for women in cannabis STEM (science, technology, engineering, and medicine). What’s your message to younger women entering a master’s program or a path toward cannabis research?
EW: Be persistent and have a thick skin. Most women find it challenging at the beginning. It’s better than it was 25 or 50 years ago, but it’s still a work in progress.
“If you include only men in studies, you’re not going to understand
— Dr. Elise M. Weerts
how it’s affecting women.”
Sunehera Hasib (CannabizMD Summer 2026): Given that women have higher CB1 receptor density and that chronic cannabis use downregulates those receptors, do you see potential in psychedelic-assisted therapies such as psilocybin to help reset receptor activity as part of cannabis-use-disorder treatment in women, especially given there’s no FDA-approved medication for CUD yet?
EW: That’s a really interesting question. I’m actually part of the group that studies psilocybin, the Center for Psychedelic and Consciousness Research here at Hopkins. I’m not aware that psychedelics act on the CB1 receptor per se, but they can affect neuroplasticity, which is genuinely interesting. My postdoc, Prachi Tiwari, PhD, studies psilocybin in both people and rodents and would be the better person to ask. It’s an exciting field, and I’m looking forward to seeing more data demonstrating that it’s safe and effective, because with any drug, you want to confirm that you’re helping and not harming the patient, that the dose works, and how many treatments are needed for the effect. All of that is still being tested in placebo-controlled trials for psilocybin, and it remains in its early stages, even more so than for cannabis.
Editor’s note. A recurring theme in this conversation was the gap between research-grade cannabis, which is standardized, tested, and placebo-controlled, and the commercial products patients actually purchase, where labeling and consistency remain unresolved. Dr. Weerts’ work also underscores that meaningful sex differences in how cannabis is metabolized and experienced are still being mapped and that rescheduling, on its own, does less to advance the science than the public narrative suggests.
MEDICAL ADVICE DISCLAIMER: This article does not provide medical advice. The information contained here is for informational and educational purposes only and is not a substitute for professional medical advice, diagnosis, or treatment. Always seek the advice of a qualified healthcare provider with questions regarding a medical condition. © 2018–2026 CannabizMD, LLC. All rights reserved.
Reference Notes
- Herrmann ES, Weerts EM, Vandrey R. Sex differences in cannabis withdrawal symptoms among treatment-seeking cannabis users. Exp Clin Psychopharmacol. 2015 Dec;23(6):415-21. doi: 10.1037/pha0000053. Epub 2015 Oct 12. PMID: 26461168; PMCID: PMC4747417. ES, Weerts EM, Vandrey R. Sex differences in cannabis withdrawal symptoms among treatment-seeking cannabis users. Exp Clin Psychopharmacol. 2015 Dec;23(6):415-21. doi: 10.1037/pha0000053. Epub 2015 Oct 12. PMID: 26461168; PMCID: PMC4747417.
- Hirvonen, J., Goodwin, R. S., Li, C.‐T., Terry, G. E., Zoghbi, S. S., Morse, C., Pike, V. W., Volkow, N. D., Huestis, M. A., & Innis, R. B. (2012). Reversible and regionally selective downregulation of brain cannabinoid CB1 receptors in chronic daily cannabis smokers. Molecular Psychiatry, 17(6), 642–649. https://doi.org/10.1038/mp.2011.82
- Spindle, T. R., Kuwabara, H., Eversole, A., Nandi, A., Vandrey, R., Antoine, D. G., Umbricht, A., Guarda, A. S., Wong, D. F., & Weerts, E. M. (2021). Brain imaging of cannabinoid type I (CB1) receptors in women with cannabis use disorder and male and female healthy controls. Addiction Biology, 26(6), e13061. https://doi.org/10.1111/adb.13061
- Vergara, D., Bidwell, L. C., Gaudino, R., Torres, A., Du, G., Ruthenburg, T. C., deCesare, K., Land, D. P., Hutchison, K. E., & Kane, N. C. (2017). Compromised external validity: Federally produced cannabis does not reflect legal markets. Scientific Reports, 7, Article 46528. https://doi.org/10.1038/srep46528
- Herrmann, E. S., Weerts, E. M., & Vandrey, R. (2015). Sex differences in cannabis withdrawal symptoms among treatment-seeking cannabis users. Experimental and Clinical Psychopharmacology, 23(6), 415–421.
- Spindle, T. R., Kuwabara, H., Eversole, A., Nandi, A., Vandrey, R., Antoine, D. G., Umbricht, A., Guarda, A. S., Wong, D. F., & Weerts, E. M. (2021). Brain imaging of cannabinoid type I (CB1) receptors in women with cannabis use disorder and male and female healthy controls. Addiction Biology, 26(6), e13061.
- Sholler, D. J., Strickland, J. C., Spindle, T. R., Weerts, E. M., & Vandrey, R. (2021). Sex differences in the acute effects of oral and vaporized cannabis among healthy adults. Addiction Biology, 26(4), e12968.
- Moore, C. F., & Weerts, E. M. (2025). Effects of sex and pre-exposure on Δ9-tetrahydrocannabinol (THC) vapor self-administration in rats. Psychopharmacology. Advance online publication.
- Moore, C., Davis, C., Sempio, C., Klawitter, J., Christians, U., & Weerts, E. (2024). Δ9-Tetrahydrocannabinol vapor exposure produces conditioned place preference in male and female rats. Cannabis and Cannabinoid Research, 9(1), 111–120.
- Weerts, E. M., Jenkins, B. W., Kuang, R. Y., Hausker, A., & Moore, C. F. (2024). Orally administered cannabigerol (CBG) in rats: Cannabimimetic actions, anxiety-like behavior, and inflammation-induced pain. Pharmacology Biochemistry and Behavior, 245, 173883.
- Elder, H. J., Zamarripa, C. A., Klausner, M., Wakshlag, J., Davis, R., Dresser, B., Kjaer, C., Weerts, E. M., Vandrey, R., & Spindle, T. R. (2025). The pharmacokinetics and pharmacodynamics of a hemp-derived ‘full-spectrum’ oral cannabinoid product (1:1 CBD:CBDA and THC:THCA). Cannabis and Cannabinoid Research, 10(2), e299–e313.
- Moore, C. F., Weerts, E. M., Kulpa, J., Schwotzer, D., Dye, W., Jantzi, J., McDonald, J. D., Lefever, T. W., & Bonn-Miller, M. O. (2023). Pharmacokinetics of oral minor cannabinoids in blood and brain. Cannabis and Cannabinoid Research, 8(S1), S51–S61.
- Spindle, T. R., Cone, E. J., Goffi, E., & Weerts, E. M. (2020). Pharmacodynamic effects of vaporized and oral cannabidiol (CBD) and vaporized CBD-dominant cannabis in male and female infrequent cannabis users. Drug and Alcohol Dependence, 211, 107937.
- Jenkins, B., Pang, C., Kuang, R., Weerts, E., & Moore, C. (2026). Effects of oral cannabidiol (CBD) on spontaneous opioid withdrawal in male and female rats. Experimental and Clinical Psychopharmacology. January 2026.
- Jenkins, B. W., Moore, C. F., & Weerts, E. M. (2025). Cannabidiol interactions with Δ9-THC on antinociception after carrageenan-induced inflammatory pain in male and female rats. Journal of Pharmacology and Experimental Therapeutics, 392(7), 103625.
- Moore, C., Jenkins, B., Cunningham, C., & Weerts, E. (2025). Targeting the endocannabinoid system for the treatment of multidimensional opioid withdrawal in rats. Drug and Alcohol Dependence, 267, 111821.
- Bedillion, M. F., Moore, C. F., Weerts, E. M., Arout, C. A., Harris, H. M., & Haney, M. (2026). Pharmacotherapy for cannabis use disorder: Preclinical and clinical models. Current Topics in Behavioral Neurosciences, 76, 249–296.
- Moore, C., Bedillion, M., Haney, M., & Weerts, E. (2025). Advancing preclinical models for medications development for cannabis use disorder: Self-administration and beyond. Current Addiction Reports, 13(1).
- Harris, H. M., Moore, C. F., Jenkins, B. W., Bedillion, M. F., Weerts, E. M., & Arout, C. A. (2026). Delta-9-tetrahydrocannabinol and cannabidiol for pain: Preclinical and clinical models. Current Topics in Behavioral Neurosciences, 76, 389–431.
- Weerts, E., Moore, C., Vandrey, R., & Jenkins, B. (2025). Evaluation of the monoterpenes alpha-pinene and limonene on sustained attention in the rodent psychomotor vigilance task. Drug and Alcohol Dependence, 267, 111615.
- Jenkins, B. W., Moore, C. F., Jantzie, L. L., & Weerts, E. M. (2025). Prenatal cannabinoid exposure and the developing brain: Evidence of lasting consequences in preclinical rodent models. Neuroscience and Biobehavioral Reviews, 175, 106207.
- Zamarripa, C., Lin, S., Slutzky, M., Antoine, D., Weerts, E., Vandrey, R., & Spindle, T. (2025). Individual and interactive effects of oral cannabis (edibles) and alcohol in healthy adults. Drug and Alcohol Dependence, 267, 111634.
- Lee, M. R., Moore, C. F., & Weerts, E. M. (2024). Oxytocin decreases alcohol self-administration in male baboons. Translational Psychiatry, 14(1), 369.




