


Rethinking cannabis policy through biology, behavior, and real-world use patterns
By Sunehera Hasib
Introduction
In his keynote for the 2021 CannabizMD Cannabis Science and Policy Forum, Cannabis & Endocannabinoid System Breakthroughs, Ethan Russo, M.D., presented findings that contribute to an evolving understanding of how and why individuals use cannabis. His research on Cannabinoid Hyperemesis Syndrome (CHS), a rare condition that causes severe vomiting in some cannabis users, found possible genetic markers that might make certain people more likely to have negative reactions. At the same time, his work on fibromyalgia explored whether dysfunction in the endocannabinoid system (ECS), a neuromodulator system involved in the regulation of mood, pain, and sleep, may play a role in chronic conditions that are not yet fully understood.
These findings, alongside Dr. Russo’s broader framework of Clinical Endocannabinoid Deficiency (CECD), suggest that cannabis use behavior may, in some cases, reflect underlying biological processes rather than solely individual choice or access to information.[1] This perspective does not replace existing behavioral or social models but expands them by introducing the possibility that biological variability influences both therapeutic use and risk.
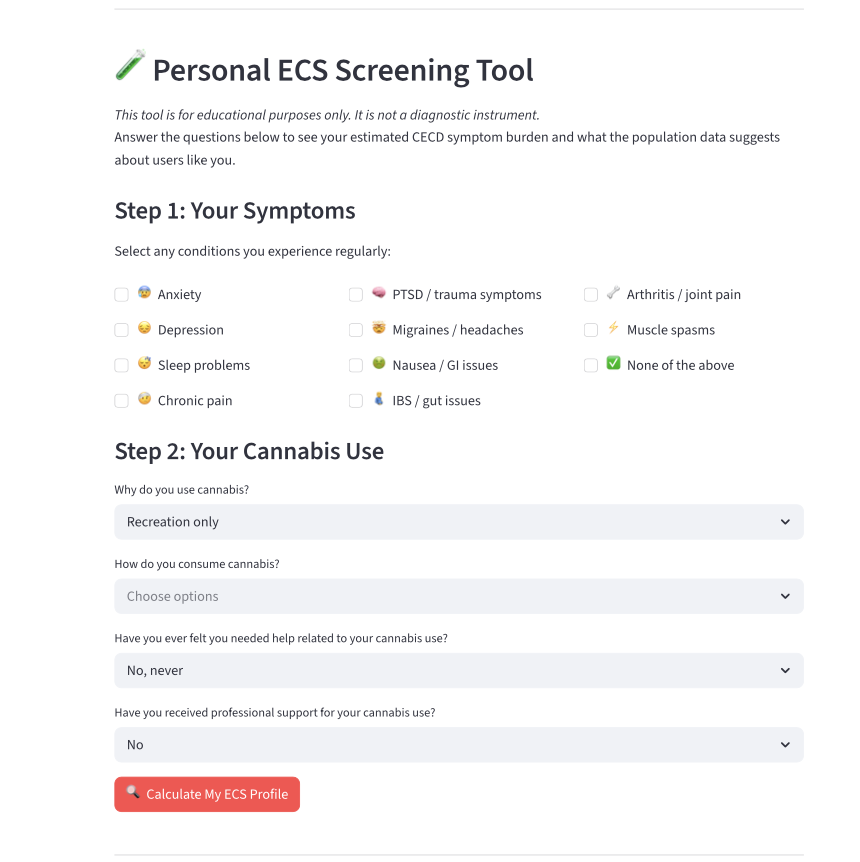
This article builds on that context through original research examining cannabis warning label recall and high-risk use patterns in a national Canadian sample, alongside the development of a public-facing Cannabis Use Disorder (CUD) Screening Dashboard.
[1] Clinical Endocannabinoid Deficiency (CECD) is a hypothesized disorder involving reduced endocannabinoid signaling (“low endocannabinoid tone”), which may underlie conditions such as migraine, fibromyalgia, and irritable bowel syndrome, as proposed by Ethan Russo.
The findings are presented as an exploration of how current policy approaches, particularly those centered on information dissemination, interact with emerging evidence from biology, behavioral science, and real-world use patterns.
Rather than framing cannabis use as a singular public health issue, this analysis considers how biological, behavioral, and structural factors intersect. Understanding this interaction may help inform more responsive approaches to cannabis policy, education, and care.
Policy Was Built on Information. The Problem Is Biological.
When Canada federally legalized cannabis for adult use in 2018 under the Cannabis Act, it built a public health framework around one core assumption: if patients or consumers know the risks, they will moderate their behavior. Mandatory rotating warning labels, standardized packaging, and public education campaigns were the primary instruments. Seven years later, general-public warning label recall have fallen from 33% to 30%, and high-risk use has not declined. However, the policy worked as designed. These findings suggest limitations in information-based approaches, more broadly to weaknesses in the underlying model of behavior change.
Dr. Russo’s CECD theory offers a critical reframe (Russo, 2011). Clinical Endocannabinoid Deficiency posits that some individuals have a constitutionally low endocannabinoid tone: a biological baseline that predisposes them to pain, anxiety, mood disorders, and poor sleep and that cannabis use addresses at a physiological level. When a person with undiagnosed CECD reads a warning label and continues using cannabis, they are not ignoring the warning. They are addressing a biological need that the warning does not cover, and that no other part of the system has identified or supported. This suggests that information-based policy approaches may be less effective for individuals whose behavior is influenced by underlying physiological factors, and that complementary models that incorporate access to care may be needed.
The United States has an opportunity to move beyond information-only models by acknowledging that cannabis use is not always a lifestyle choice but may reflect underlying health conditions. Policy frameworks that better integrate emerging scientific evidence may be more responsive to these realities.

Warning Label Recall Predicts Greater High-Risk Use — Not Less
Using machine learning applied to a national Canadian sample, this research found that individuals who recalled cannabis mental health warning labels were systematically more likely to report high-risk cannabis use, not less (Hasib et al., 2026). This counterintuitive finding serves as the empirical foundation of everything that follows. The standard policy model assumes a linear chain: mandate a warning, increase recall, change behavior, reduce harm. The data breaks that chain at the second link. Recalls and behavior changes are different, and in high-risk populations, they may even lack correlation. Research by Dr. Ethan Russo on genetic variability in cannabis responses further supports that high-risk users may represent a biologically heterogeneous population.
“Warning labels assume the problem is a lack of information. Endocannabinoid science tells us the problem is often a lack of care. You cannot fix a biological gap with a sentence on a package.”
The mechanism is not mysterious. High-risk users buy more cannabis, use it more often, and thus encounter product packaging more frequently than low-risk users. They see the warnings more because they use more cannabis, not because the warnings are protectively reaching them. But there is a deeper layer here that Dr. Russo’s work illuminates: some of these high-risk users are managing genuine biological needs. These needs may include endocannabinoid deficiency and a genetic susceptibility to certain adverse effects they are not aware of, or psychiatric conditions being partially addressed by cannabis; then a warning label is not an intervention. It is a speed bump. What these individuals need is not only a better label. They need a clinician who understands the endocannabinoid system, a screening tool that identifies their specific risk profile, and a system that meets them where they are. Current practice limits such systems, presenting a potential area for development.

The mechanism is not mysterious. High-risk users buy more cannabis, use it more often, and thus encounter product packaging more frequently than low-risk users. They see the warnings more because they use more cannabis, not because the warnings are protectively reaching them. But there is a deeper layer here that Dr. Russo’s work illuminates: some of these high-risk users are managing genuine biological needs. These needs may include endocannabinoid deficiency and a genetic susceptibility to certain adverse effects they are not aware of, or psychiatric conditions being partially addressed by cannabis; then a warning label is not an intervention. It is a speed bump. What these individuals need is not only a better label. They need a clinician who understands the endocannabinoid system, a screening tool that identifies their specific risk profile, and a system that meets them where they are. Current practice limits such systems, presenting a potential area for development.
The 20–24 Age Group Is the Highest-Risk Window and the Highest-Opportunity Window
Adults aged 20 to 24 represent the highest cannabis use rates of any age group in both Canada and the United States. The 2024 NSDUH found that approximately one in three young adults aged 18 to 25 used marijuana in the past year.[1] This is also when the brain is developing the most; the prefrontal cortex and endocannabinoid system are still growing until about age 25, which is exactly when Dr. Russo’s research shows that the risk of negative reactions is highest for those who are genetically more likely to have issues with cannabis. Young adults in this range are not simply choosing high-risk behavior. Some are biologically more susceptible to cannabis-related harms than they or any clinician would know without genetic screening or a detailed symptom history. This period of vulnerability aligns with Dr. Russo’s findings, emphasizing the role of endocannabinoid system maturation in early adulthood.
Notably, this demographic is also the most educationally responsive cohort. Research on health behavior change consistently shows that young adults aged 20 to 24 are more likely to modify behavior when given clear, relevant, community-embedded information—not abstract warnings on packaging, but engaged education in spaces they trust. Community education events, such as those hosted by nonprofit The Tea Pad Foundation, represent the kind of engagement that effectively reaches this population. Dispensary visits, community events, and peer conversations: these are the touchpoints that shift behavior in this age group. The CUD Screening Dashboard was designed to fit into exactly these moments: brief, non-stigmatizing, free, and connected to support. This intersection is where science and social justice meet in practice.
[1] In this article, the terms “cannabis” and “marijuana” are used in context-specific ways. “Marijuana” reflects terminology used in national datasets such as the National Survey on Drug Use and Health (NSDUH).

Dispensaries Are the Most Underutilized Public Health Access Point in Cannabis
Canada’s legalization created broad, federally regulated retail access to cannabis without building any clinical support infrastructure alongside it. The result is a country where cannabis is available on every street and where most medical cannabis users report using it without documentation from a healthcare professional. Most clinicians are not trained on the endocannabinoid system at scale, reflecting broader gaps in cannabis workforce training and patient-facing education, particularly in dispensary settings (Cohen Roth, 2019). In Canada, pharmacists are not integrated into the dispensary model. Genetic screening for CHS susceptibility or cannabinoid receptor abnormalities, such as those Dr. Russo is pioneering, was not included in any access pathway. In the Canadian market, people walk in, buy their cannabis products, and leave, with the warning label on the package remaining the primary public health intervention.
Dispensaries represent a consistent point of contact with individuals who use cannabis, often during the early stages of use patterns that may benefit from brief intervention or guidance toward safer use. In the United States, they are also one of the few cannabis-adjacent environments where workforce development efforts intersect with public health objectives.
However, structural constraints shape their capacity to serve this role. Under Section 280E of the U.S. Internal Revenue Code, cannabis businesses are unable to deduct most ordinary business expenses, resulting in comparatively high effective tax burdens (Cohen Roth, 2019). This financial framework can limit investment in staffing, training, and consumer-facing health services.
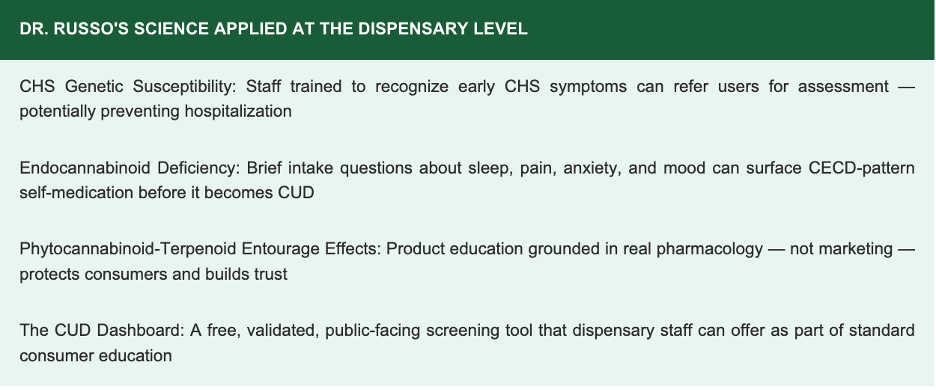
Within these constraints, there remains an opportunity to expand the role of US dispensaries through low-barrier, evidence-informed approaches. For example, training staff to offer brief Cannabis Use Disorder (CUD) screening tools grounded in validated instruments, informed by endocannabinoid system research, and connected to community-based resources may not function as a clinical intervention but rather as an extension of public health infrastructure.
Such approaches may offer a cost-efficient way to increase early identification of risk, improve access to information and support, and reach individuals at a point of regular engagement. In communities historically underserved by both healthcare systems and the regulated cannabis industry, these touchpoints may also advance health equity by improving access to guidance and care.
Unsupervised Psychiatric Medication Substitution is An Underexamined and Potentially Significant Issue
Among the most urgent findings in this research is the direct measurement of a pattern that the healthcare system has no current mechanism to detect individuals replacing prescribed psychiatric medications, such as antidepressants, anxiolytics, and sleep medications, with cannabis without clinical awareness or oversight. This phenomenon was not inferred. It was directly measured in a national Canadian sample. No physician was notified. No treatment plan was adjusted. The medication was simply stopped, and cannabis substituted. In a country where medical cannabis is federally legal and available to virtually anyone who presents a health need, this pattern is not a fringe phenomenon. The entire warning label infrastructure was not designed to address this quiet, widespread practice.
Dr. Russo’s work gives the current finding a biological dimension that makes it more urgent, not less. If CECD underlies some of the conditions for which these individuals were originally prescribed psychiatric medications for anxiety, depression, sleep disorders, and pain, then cannabis substitution may be a partially effective biological self-correction happening outside any clinical relationship. The concern is less the act of substitution itself and more the absence of clinical oversight. Without dosing guidance, without monitoring adverse reactions, without knowledge of their own potential genetic susceptibilities, and without anyone in the system even knowing it is happening, cannabis substitution may occur without any clinical oversight. This invisibility is compounded for Black and Brown communities that already face higher rates of untreated mental illness, more barriers to psychiatric care, and deeper mistrust of medical institutions. The CUD Screening Dashboard is one tool for making risk visible—safely and voluntarily through a free, public-facing online platform accessible via mobile or desktop and available in dispensary settings, community education events, and other points of engagement.
Study Limitations
The author’s analysis is subject to several limitations. The findings rely on self-reported data, which may introduce recall or reporting bias. Additionally, the results are observational in nature and therefore do not establish causality. The Clinical Endocannabinoid Deficiency (CECD) framework remains an evolving scientific theory and has not yet been fully validated in clinical settings. Finally, genetic screening for cannabis-related susceptibility is not yet widely implemented, limiting the ability to apply these insights at scale.
Conclusion: From Warning Labels to Whole-Person Care
Dr. Russo’s 2021 CannabizMD Forum keynote concluded with a vision: evidence-based cannabis therapeutics grounded in genetics, endocannabinoid science, and the plant’s real pharmacology. The five findings in this article trace what happens when that vision has not yet been realized at the policy level, when people are left to self-manage a complex biological relationship with cannabis in a system that hands them a warning label and calls it public health.
“The science is advancing, and communities are engaging with these issues in real time.
Policy has an opportunity to evolve alongside them.”
Canada’s experience with information-based approaches highlights potential gaps in current models. The United States has an opportunity to build on these lessons by exploring more integrated frameworks that support dispensary staff as part of a broader public health ecosystem, incorporating validated digital screening tools to identify risk earlier, and engaging emerging scientific understanding of the endocannabinoid system in clinical and educational contexts.
Such approaches may also benefit from prioritizing equitable access to resources and support, particularly for communities disproportionately affected by past cannabis policies. This direction aligns with the broader goals of education-focused organizations such as CannabizMD. It reflects the intent of this research: to contribute to ongoing discussions on more responsive, evidence-informed cannabis policy.
Sunehera Hasib is a cannabis policy researcher and developer of the Cannabis Use Disorder (CUD) Screening Dashboard. She can be reached at shasib@gmu.edu.
Editor’s note: This content is for educational purposes only. Content does not constitute medical advice and may not reflect the official positions of CannabizMD LLC. Consult a qualified healthcare provider for medical guidance.
References
Hasib, S. et al. (2026). Chasing the High: Cannabis Mental Health Warning Label Recall is Associated with Greater, Not Lesser, High-Risk Use in a National Canadian Sample. OSF Preprints. https://doi.org/10.31235/osf.io/znrhe_v1
Russo, E.B. (2021). Cannabis & Endocannabinoid System Breakthroughs. CannabizMD 2021 Cannabis Science and Policy Forum Keynote. CannabizMD YouTube Channel.
Russo, E.B. (2011). Taming THC: Potential Cannabis Synergy and Phytocannabinoid-Terpenoid Entourage Effects. British Journal of Pharmacology, 163(7), 1344–1364.
SAMHSA. (2025). Key Substance Use and Mental Health Indicators: Results from the 2024 NSDUH. U.S. Department of Health and Human Services.
Choi, N.G. et al. (2024). Cannabis use disorder and substance use treatment among U.S. adults. Journal of Substance Use & Addiction Treatment, 167, 209486.
Health Canada. (2024). Canadian Cannabis Survey 2024: Summary. Government of Canada.
Meek, C.J. et al. (2024). Regulatory Landscape of Cannabis Warning Labels in US States. American Journal of Public Health, 114(S8), S681–S684.
CannabizMD. (2025). About CannabizMD. https://www.cannabizmd.com
Tea Pad Foundation. (2025). Meet Tea Pad. https://teapad.co/meet-tea-pad
CUD Screening Dashboard (2024). https://cannabis-public-cudscreen-dashboard-2v4suvungmct9p73mfa5hq.streamlit.app/
Jacquie Cohen Roth (2019). How a lack of dispensary attendant training puts patients at risk. CannabizMD. https://www.cannabizmd.com/uncategorized/compliance-uncategorized/hr/how-a-lack-of-dispensary-attendant-training-puts-patients-at-risk/
Jacquie Cohen Roth (2019). Understanding cannabis tax laws. CannabizMD. https://www.cannabizmd.com/uncategorized/compliance-uncategorized/finance-accounting/understanding-cannabis-tax-laws/




